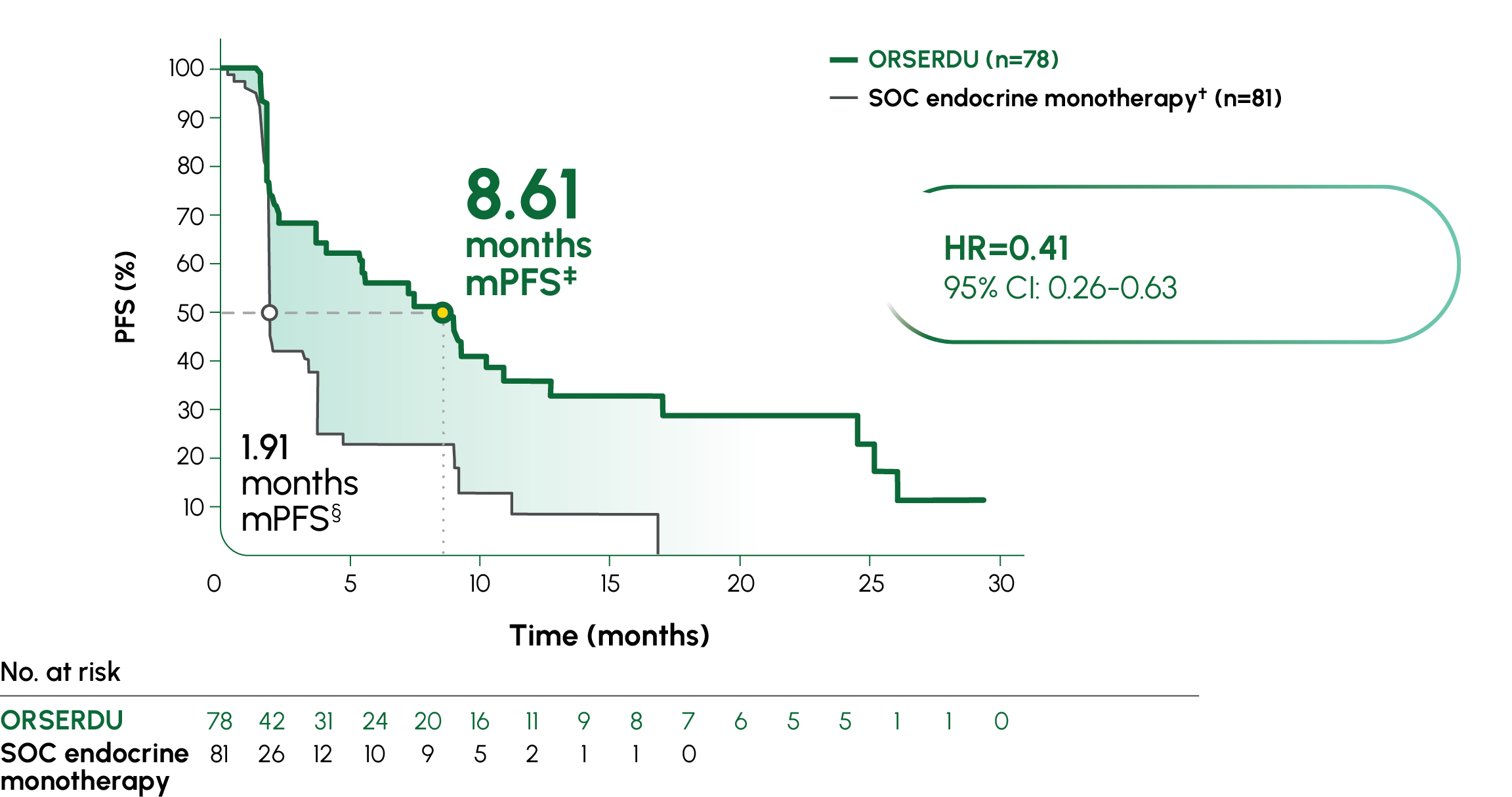
PRIMARY ENDPOINT IN EMERALD: PFS IN PATIENTS WITH ESR1-MUTATED mBC1
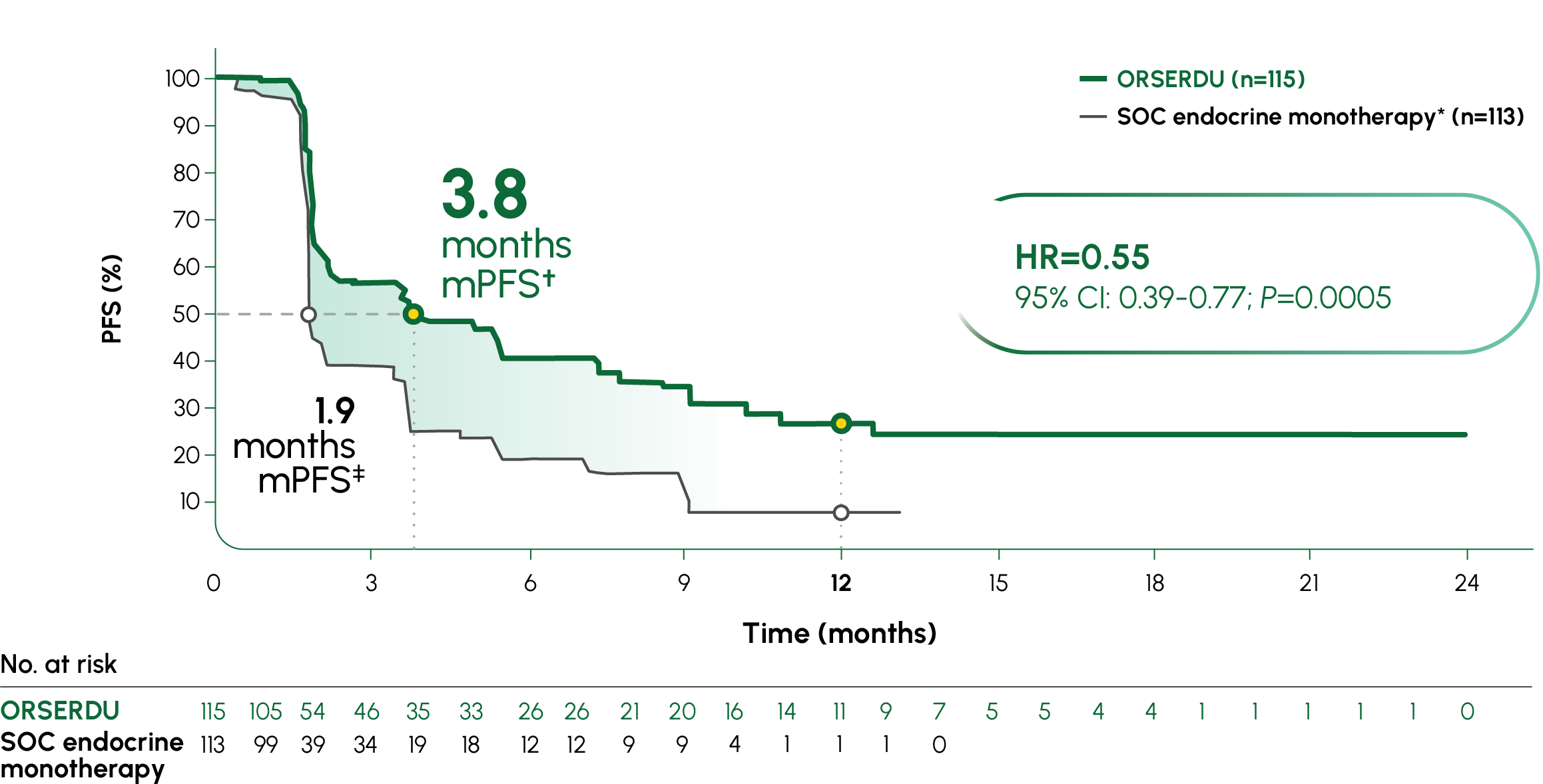
Absolute difference in mPFS of 1.9 months between SOC and ORSERDU arms1
In EMERALD, 73% in the SOC arm were treated with fulvestrant3
In a post hoc analysis, patients on fulvestrant achieved 1.9 months mPFS, while patients on ORSERDU achieved 3.8 months3
Post hoc analysis data are observational in nature. There was no prespecified statistical procedure controlling for type 1 error.
Due to low bioavailability, fulvestrant is only available as an IM injection5,6
Fulvestrant is not indicated to treat ESR1-mutated disease5
CDK4/6i, cyclin-dependent kinase 4/6 inhibitor; CI, confidence interval; ER+, estrogen receptor-positive; ESR1, estrogen receptor 1; ET, endocrine therapy; HER2-, human epidermal growth factor receptor 2-negative; HR, hazard ratio; IM, intramuscular; mBC, metastatic breast cancer; mPFS, median progression-free survival; PFS, progression-free survival; SOC, standard of care.
*mPFS was the primary endpoint. SOC endocrine monotherapy included either fulvestrant, anastrozole, letrozole, or exemestane.1
†95% CI: 2.2-7.3.1
‡95% CI: 1.9-2.1.1
Selected Important Safety Information
Warnings and Precautions
Dyslipidemia: Hypercholesterolemia and hypertriglyceridemia occurred in patients taking ORSERDU at an incidence of 30% and 27%, respectively. The incidence of Grade 3 and 4 hypercholesterolemia and hypertriglyceridemia were 0.9% and 2.2%, respectively. Monitor lipid profile prior to starting and periodically while taking ORSERDU.
Please see additional Important Safety Information below. Please see full Prescribing Information.